
 English
English  Português
Português  Español
Español by Alberto J. Muniagurria - Eduardo Baravalle
The interrogation is a method that consists of taking the subjective and objective data of the patient and transcribing them correctly, with the appropriate language and with impartiality; It also implies knowing how to present them in a concrete and precise way, without giving rise to ramblings or additional explanations.
The physical exam is an art that is learned by repeating its practice. Despite the fact that there are different methods or techniques to carry out this practice, it is convenient, for those who start, to internalize themselves in the techniques that have acquired value over the years. Once these maneuvers are known, in the daily medical activity, those that best suit the observer's preference or possibilities can be selected.
Likewise, it is important to remember that the doctor or observer must perform all the maneuvers in the medical history, both during the interrogation and the physical examination, with a professional attitude.
The best way to learn the physical exam is through supervised practice. Because it is a manual activity, it is easier to acquire with practice than with study. As medical knowledge is incorporated, the execution of the maneuvers will improve, due to the understanding of what is intended to be found. The physical examination data should always be evaluated in the general context of the patient, and not as single and isolated findings.
In the physical examination, a methodology and order of work must be established. Some principles need to be clear. What is the usefulness of the physical examination? What information should you look for? What mistakes can be made? What accessories should be used in the physical examination? Today it is known that more than 50% of etiological diagnoses arise from the study of the clinical history, and in turn it must be recognized that the highest percentage of errors appear due to an incorrect or incomplete physical examination. Regarding the information that is required to search, that is, the changes that the disease produces in the organism and that are manifested through the signs or objective data, it is necessary that previously it is known what is normal. Nor should it be forgotten that normality is subject to change; a normal physical exam does not mean that normality will always be maintained in subsequent exams. Therefore, it is important to repeat the exam as many times as the situation requires.
Since the physical examination uses the senses (sight for inspection, touch for palpation and hearing for percussion and auscultation) that are being perceived through consciousness, with the errors that may arise from the limitation of these methods, there must be an objective and balanced behavior, recognizing normality with its variants, to differentiate or distinguish abnormal events. It is essential that there be concentration to be able to develop the correct technique following a working method that does not vary with the different patients, to avoid the omission of findings and to be able to describe the signs in an identical way to another observer. The physical examination must be carried out in an orderly and complete manner; sometimes it can be directed by the questioning towards the diseased organ or the symptom, without losing an objective attitude in search of abnormalities. In other words, the observation of the signs in the physical examination must be complete, orderly, objective and reproducible.
Then some points of interest to the observer have been seen. Some considerations will now be presented from the point of view of the observed. It is easy to imagine all the reasons a patient may have for anxiety and fear about the physical exam. To minimize this unpleasant sensation that is caused and to have a total cooperation of the patient, certain elements that must be known are necessary.
The observer's attitude to the physical examination should be calm and patient, but firm; All the maneuvers to be performed and what is requested of him must be anticipated in a clear and concrete manner. It is necessary to convey the feeling of a regulated routine to which he will adapt naturally.
Physical exam
We must try to make the most of the positions that the patient is acquiring to avoid continuous changes and increase the efficiency and speed of the examination. All the elements to be used should be at hand.
The physical examination is carried out with the patient on the examination table or stretcher or on his bed when he is hospitalized or at home. It is done routinely after questioning. The physical examination consists of four successive steps, which vary in their order of application according to the apparatus being examined, and which consist of inspection, palpation, percussion, and auscultation. The doctor applies all his senses to, through them, obtain information about the static and dynamic facts of the human body.
The examination actually begins when the patient enters the office or when he is first observed in his bed, the information given by the expression of his face, the color of the skin and mucous membranes, and the shape and structure of their anatomy, provide useful data. By shaking hands, contact is made with the patient, and it will be possible to appreciate their firmness or weakness, humidity or dryness, facts that will contribute to the final assessment of the individual.
To carry out a thorough and thorough physical examination, a series of factors or elements of great importance should be taken into account so that the information obtained is as complete as possible.
1. Environment. It should be spacious enough to include a desk with a chair for the doctor and two for the patient and a family member. It will also have a stretcher with sufficient height to allow obtaining the desired positions comfortably and in turn, to be able to carry out special practices, such as rectal examination or vaginal examination. It should be possible to circulate around the table to exercise the maneuvers, both to the right and to the left of the patient, even though the examiner will perform better the maneuvers on the right side of the patient.
In addition to the stretcher, it is convenient to have a table or shelf where the necessary instruments for a complete physical examination will be supported.
The room should be insulated from noise as much as possible with an appropriate and quiet ventilation, heating and cooling system. The temperature will be comfortable to allow a correct examination of the patient, without awakening a feeling of cold or excessive heat. The patient is explored with the least amount of clothing possible; covered, to protect your modesty. The lighting should be natural and direct light. It should also have a sink and a dressing room.
2. Instrumental. The doctor will use a series of instruments for the physical examination that will collaborate in obtaining data about the patient:
- Balance
- Tensiometer
- Stethoscope
- Thermometer
- Ophthalmoscope
- Otoscope
- Rhinoscope
- Flashlight
- Disposable tongue depressors - Reflex
hammer
- Tuning fork from 128 to 256 cycles per second
- Pins
- Cotton and alcohol
- Gloves
- Vaseline or creams commonly used in treatments of hemorrhoids
Inspection. It is to recognize with attention; involves prior knowledge provided by theoretical knowledge and prior experience.
Inspection is the method that allows obtaining direct information on the shapes, sizes, limits, coloration, surface, mobility, attitude, level of consciousness, habit, sexual development, facial expression (given by the muscular movements of the face) and movements of the Body. It should not only be performed on the patient, but also by observing the people who accompany him, since, if they are linked by blood ties, they can present similar anomalies.
Inspection begins when the patient enters the room, is maintained during questioning, and is part of the entire physical examination. It is also done on their clothes, which can provide information about the personality of the individual, their tastes, their hygienic habits, their customs. The absence of normal situations or the presence of abnormal situations should attract the observer's attention.
The patient must be devoid of his clothes, defending his modesty with a cloth that will be running successively according to the area to be explored. Lighting must be perpendicular, preferably natural light. When it is desired to observe movements, the light will be tangential, which is useful, for example, in the examination of the heartbeat.
The inspection is carried out both on the surface and with the help of special instruments, which allow the observation of deep structures.
 Palpation. It consists of touching something with your hands to recognize it through the sense of touch.
Palpation. It consists of touching something with your hands to recognize it through the sense of touch.
Palpation begins, as already mentioned, by shaking hands with the patient. Through palpation, information is obtained on the shape, size, limits, consistency, surface and humidity, sensitivity, mobility induced by palpation and temperature, and it also allows evaluating whether the palpated structure constitutes part of surface formations or if it is located in the depth. When internal structures such as the mouth or rectum are palpated, the maneuver is called touch.
Palpation is done with the observer's right hand, or with both hands if the examination is bimanual. Unimanual palpation (Figure 2-1) can be superficial or deep, and is performed by trial and error flexing the metacarpophalangeal joints.
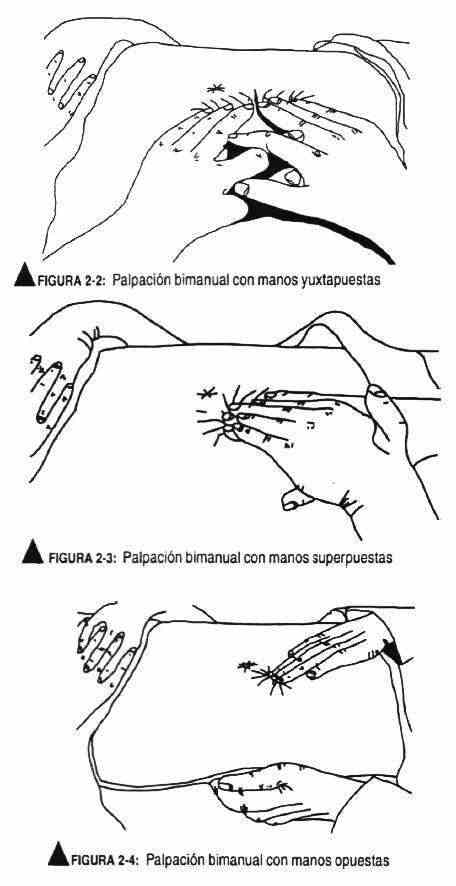
In the bimanual examination, in general, one hand helps or collaborates with the other, fixing organs or structures.
The bimanual examination can be with juxtaposed hands, overlapping hands, or opposite hands. With juxtaposed hands (Figure 2-2), it consists of the overlapping of the thumbs and index fingers, to expand the palpatory surface.
Overlapping palpation (Figure 2-3) involves placing one hand on top of the other, and is used for deep organ palpation; one hand presses and the other palpates. Opposing palpation (Figure 2-4) is intended to bring the organ to be palpated closer to the other hand.
 Shape: The shape should be described according to its geometric characteristics and not because of its resemblance to known structures. Example: it should be said in a rounded way and not "like an orange".
Shape: The shape should be described according to its geometric characteristics and not because of its resemblance to known structures. Example: it should be said in a rounded way and not "like an orange".
Size: It must be expressed in centimeters or millimeters, in its largest and smallest diameters. Example: 5 cm in its largest horizontal diameter and 3 cm in its vertical diameter, and not "the size of a tangerine."
Limits: It will be specified if the limits are net or diffuse, the latter in the event that they are confused with neighboring structures.
Consistency: The consistency varies from soft to stony, through elastic and fibrous.
Surface: The surface must be described in terms of whether or not there are irregularities or nodulations.
Humidity: The humidity of the skin, together with the tonism, are related to the hydration status of the patient.
Sensitivity: Palpation can cause pain, which is normal at the level of certain viscera (breasts, aorta, testicles). Also by palpation it is possible to discover hypoalgesic areas.
Mobility: In this aspect, the presence or absence of mobility on deep and superficial planes, spontaneous, respiratory, digestive and neurological movements, fetal beats, etc., which must be carefully recorded, will be described.
Temperature: It is obtained by supporting the back of the fingers that explore with the surface to be palpated. In addition, a comparative estimation must be made in the case of symmetric structures.
Percussion. It consists of hitting or striking the area to be explored to produce noises and vibrations that define certain characteristics of the underlying structures. The objective of this technique is to recognize the sound and / or vibratory characteristics of a given area, thus allowing the limits of the organs to be defined. The increase or decrease, or the absence or variation of the usual sounds suggests the existence of abnormal findings on examination. Comparative symmetric-sided percussion is also used to investigate whether the sound quality is equal. Percussion is a more precise technique than palpation to define the size of the organs.
Percussion can be direct or indirect. It is direct when performed with two or three fingers of the hand (index, middle and ring) that strike on the surface to be studied, and it is used to strike bones, such as the dorsal spine, or to have a general notion of loudness thoracic. It is indirect when using a pleximeter finger (Figure 2-5) and a hammer finger (Figure 2-6). The pleximeter finger rests on the surface to be explored while the hammer finger hits the pleximeter finger, thus obtaining the sound (figure 2-7)
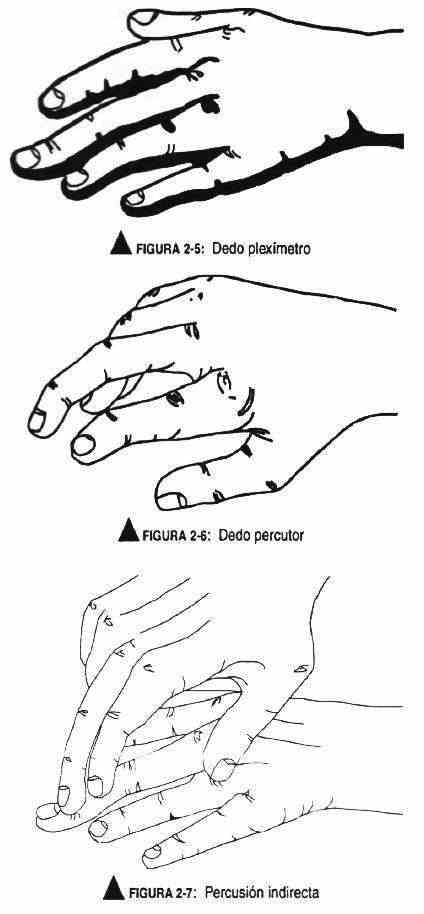 The pleximeter finger is the middle finger of the left hand; the other fingers of this hand should be raised to prevent them from modifying the sound obtained by braking the vibrations induced by the blow. The striker finger is the middle finger of the right hand that, partially flexed, executes a sharp and rapid blow through a movement of the wrist. It is struck with the tip of the finger and not with the ball of the foot. For a better execution of the maneuver the nails should be trimmed.
The pleximeter finger is the middle finger of the left hand; the other fingers of this hand should be raised to prevent them from modifying the sound obtained by braking the vibrations induced by the blow. The striker finger is the middle finger of the right hand that, partially flexed, executes a sharp and rapid blow through a movement of the wrist. It is struck with the tip of the finger and not with the ball of the foot. For a better execution of the maneuver the nails should be trimmed.
The shocks should not be intense, but sufficient to obtain a clear sound, and appropriately separated from each other to avoid overlapping vibrations.
Through percussion different sounds are obtained depending on whether it is a solid parenchyma, partitioned air or open air.
In this way, different qualities of sounds can be obtained: matte, submate, tympanic, voiced and hypersonous (Table 2-1). Dullness is the soft, muffled, muffled sound with a high timbre and short duration, typical of solid organs and liquid collections. The typical loudness of normal lung fields (septate air) is characterized by a high, prolonged, low-pitched sound. Bloat (open air), which is a sound similar to that of the drum, is intense, with a musical timbre, typical of the gastric chamber.
Table 2-1. Type of sounds that are obtained with percussion |
||
| Sound type | features | Location |
| Mate | Soft, muffled, muffled, high timbre, mid-high frequency, short duration | Solid organs and liquid collections |
| Sonorous | Low frequency, low tone, prolonged | Lung |
| Tympanic | Intense, musical | Gastric chamber |
| Hypersonoro | Very intense, low frequency | Pneumothorax, emphysema |
Submatidity occurs, for example, when the lung reed is percussed on the liver; hypersonority is louder than loudness, without reaching bloat, and is characteristic of pneumothorax or emphysematous chest
Auscultation. It is the method that allows you to listen to the sounds that are produced in the body spontaneously; can be immediate or direct or indirect, using a stethoscope (Figure 2-8)
The tone is the frequency of vibration, it is the greater or lesser elevation of the sound produced by the greater or lesser speed with which the sound bodies vibrate. The timbre is the typical sound of an object, given by the characteristics of its material; it has a dominant vibration, along with minor ones, called overtones, which can be harmonics. Intensity is the amplitude or height of the vibrations; the greater the energy and the lower the rigidity of the vibratory system is greater.
Sound is the sum of vibrations of a dominant frequency or fundamental tone, plus vibrations of a multiple frequency of the fundamental tone, known as harmonic overtones. Also called fundamental sound. When the tone or frequency of vibration is uneven, irregular, with disharmonic tones, it is called noise. In the cardiac cycle, the Spanish terminology designates normal valvular auscultatory phenomena by the name of noise, while the Anglo-Saxon terminology refers to sounds.
 Stethoscope: It is one of the most useful and important instruments available to a modern doctor. Stethoscopes vary significantly in quality and efficiency. The doctor should choose the stethoscope that provides the most information taking into account the following factors:
Stethoscope: It is one of the most useful and important instruments available to a modern doctor. Stethoscopes vary significantly in quality and efficiency. The doctor should choose the stethoscope that provides the most information taking into account the following factors:
- Ability to detect murmurs and low noises and in turn the softest high frequency murmurs.
- The olives should be neither too tight nor too loose, and they should be the best size to suit the observer's ear canal. If they are very small and tight, they will penetrate the canal causing pain and distracting attention. Its angulation must also be taken into account, which influences the adaptation of the ear canal.
- The rubbers must be flexible and as short as possible, approximately 25 cm, and with the best conditions for the transmission of murmurs and noises. They should not hit each other during the maneuver, because these blows disturb auscultation.
- They must have a membrane (diaphragm) and a bell. The diaphragm takes the highest frequencies, and therefore it is desirable to be rigid. The bell picks up low-frequency sounds, such as the third and fourth noises. The stethoscope head must be weighted enough to hold the bell in position without causing excessive compression. By progressively compressing the bell on the precordium, the skin stretches and picks up the sharpest vibrations, that is, the skin begins to function as a membrane. Therefore, for sounds or murmurs or low-pitched or bass noises, the contact on the skin must be very soft. This maneuver can be useful when you want to differentiate a high frequency sound from a low frequency one.